
Sarah Solomon
Abstract
The complex consequences for healthcare delivery prompted by the effects of coronavirus disease 2019 (COVID-19) on the general population are not yet fully understood. At the time of writing, there are only five meta-analyses and literature reviews, the most comprehensive of which includes a total of 32 papers. Of these five reviews, four focus on telehealth and only one on personal protective equipment (PPE) (Anthony Jnr, 2021; Chaudhry et al., 2021; Galanis et al., 2021; Gao et al., 2020; Monaghesh & Hajizadeh, 2020). There is furthermore a scarcity of research on the impact that these COVID-19 healthcare delivery changes may have on patients with physical and/or intellectual disabilities; no meta-analyses or related reviews on this matter have been published. This at-risk group has experienced adverse short-term effects, but potentially favorable long-term outcomes, due to four major pandemic-related healthcare delivery modifications: (1) the widespread proliferation of telemedicine, (2) increased use of personal protective equipment (PPE), (3) COVID-19 testing requirements and (4) patient-physician relationship (PPR) adjustments. All four of these modifications have complicated the ability of the special needs population to access medical care in the immediate term. However, some consequences of COVID-19 – especially the growth of telemedicine and the resultant transformations in PPR dynamics – may generate lasting beneficial changes in how the healthcare system interacts with the disabled community.
Download PDF
Roundtable Journal on Health Policy | Volume 3 | Issue 2
Full Text:
Coronavirus disease 2019 (COVID-19) has been deeply disruptive in numerous ways, with life-changing consequences for social cohesion, economic activity, and mental and physical health in the United States. However, the pandemic’s effects on certain segments of the population appear more mixed, suggesting that a deeper analysis is necessary to fully explore the implications. For individuals with physical and/or intellectual disabilities, COVID-19 has resulted in mixed outcomes, ranging from exacerbations of preexisting problems to the potential for beneficial changes in the field of special needs medical care. As an often-forgotten, at-risk group, members of the special needs population – although diverse in diagnosis, symptom presentation and comorbidities – possess unique healthcare risks that require intensive care (Boyle et al., 2020; Jeste et al., 2020; Robinson et al., 2003). People with disabilities are particularly vulnerable to the pandemic’s impact on healthcare delivery since they use health services at high rates, may require in- home medical care, and need specialty- specific providers (Aishworiya & Kang, 2020). Furthermore, families of special needs patients have reported feeling under- considered during the implementation of many COVID-19 changes. This is due in part to a lack of studies assessing this population’s needs during the pandemic (Boyle et al., 2020; Jeste et al., 2020; Lebrasseur et al., 2021).
There are four main healthcare delivery changes that have occurred as a result of the pandemic: (1) an increase in telemedicine services; (2) interaction through personal protective equipment (PPE); (3) COVID-19 testing before/during medical visits (Lapow, 2020); and (4) the combined effect of telemedicine and PPE on the patient- physician relationship (PPR). All of these changes have had varying short-term and potential long-term effects on healthcare delivery to the special needs community.
(1) Telemedicine
Telemedicine existed before the pandemic, but was not well established, widely used, or easily accessible and reimbursable. The barriers to using telemedicine included technological limitations, insurance coverage, and doubts about its efficacy. However, the emergence of COVID-19 required rapid changes to overcome obstacles caused by the need for social distancing, a shortage of healthcare workers, and overwhelming patient volume (Lapow, 2020; Mann et al., 2020). A useful analogy can be found in higher education, where online services were available pre- pandemic – even well-established at a number of institutions – but have since boomed in response to the changing environment (Teräs et al., 2020). The surge in COVID-19-related telemedicine was similarly built upon an already existing but less robust infrastructure (Lapow, 2020; Mann et al., 2020). Furthermore, like telemedicine, the increase in online education has impacted different types of students in varying positive and negative ways: for example, adult students with young children may save money on childcare but may be less able to concentrate on their online classes due to a distracting home environment (Teräs et al., 2020).
While COVID-19 has resulted in the widespread use of telemedicine, this tool had already been studied prior to the pandemic as a form of care for patients with disabilities. Before 2020, telemedicine was investigated as a means of improving disability care, which is centered around a close working relationship between families and multiple different healthcare groups. Telemedicine was shown to improve this linkage, as more family members of patients were informed of and held accountable for executing plans of care. In the typical in-person scenario, one or two family members accompany their relative for on-site visits. Virtual telemedicine visits allow the entire family to attend a consultation. In addition, families now have access to highly experienced special needs providers irrespective of distance or available means of travel (Robinson et al., 2003). However, for this benefit to remain after the pandemic, legislation revoking cross state- line care restrictions will need to be implemented (Annaswamy et al., 2020).
Another pre-COVID-19 telehealth study also found that approval ratings of telemedicine by both disabled patients and their physicians increased over time as both groups became more comfortable with the platform and gradually adapted to the change (Karp et al., 2000). However, the hurried switch from face-to-face to online healthcare delivery triggered by the pandemic is likely to produce a J-shaped curve regarding the ratings of telemedicine, as this change did not allow time for many of these patients to fully adjust. This issue especially pertains to individuals with intellectual disabilities who attend weekly routine healthcare visits and require a very strict schedule to function properly. Without ample time to adapt, these individuals initially experienced adverse repercussions from the switch to telemedicine (Constantino et al., 2020; Eshraghi et al., 2020; Neece et al., 2020).
For persons with physical disabilities, the overall cost of visits may have decreased in terms of travel and medical care, depending on insurance plan (Annaswamy et al., 2020; Constantino et al., 2020; Lapow, 2020). The rapid and intense nature of the pandemic caused insurance companies to reevaluate telemedicine as a valid medical necessity, which will be a major benefit for special needs families that intend to utilize these services post-COVID-19 (Hooshmand & Foronda, 2017; Karp et al., 2000; Lapow, 2020; Robinson et al., 2003). A 2017 study by Hooshmand and Foronda reported that the cost of telemedicine versus a local office visit was about the same at $55. However, local special needs providers are frequently not available, and in these cases families must travel outside of their community to access care, raising the cost of an in-person visit to about $197. These findings suggest that telemedicine is significantly more cost- effective for the special needs population, assuming adequate insurance coverage (Hooshmand & Foronda, 2017). In one US study examining the special needs population, 51.6% (n = 669) lost at least one medical service due to a COVID-19-related decrease in in-person healthcare delivery (Jeste et al., 2020). Despite improvements in telemedicine technology, a complete lack of in-person visits is not in the best interest of this community (Annaswamy et al., 2020; Eshraghi et al., 2020). Many families of individuals with severe physical and/or intellectual disabilities also require in-home health services and have reported a significant reduction in these benefits, such as home-based physiotherapy, nursing services, day- and nighttime health aids, etc. (Boyle et al., 2020; Constantino et al., 2020; Jeste et al., 2020; Lebrasseur et al., 2021). Post-pandemic, the special needs community will likely require a balance of in-person and virtual consultation.
(2) Personal Protective Equipment (PPE)
PPE is designed to limit the spread of disease by acting as a barrier against infectious agents. The effect of PPE on the interaction between patient and provider will be discussed in the section on PPR. The emphasis here is on the requirement that masks be worn when attending in-person healthcare visits. The few available studies mainly focus on the effects of masks in everyday life without considering their impact on healthcare delivery. Moreover, persons with disabilities will have varying reactions to and impairments from wearing a mask. (Pendo et al., 2020). Five such reactions will be addressed here. (A) Individuals with touch sensitivities, the most common type being autism spectrum disorder (ASD), may have their symptoms exacerbated by mask requirements during healthcare visits. (Kohek et al., 2020; Pendo et al., 2020; Sivaraman et al., 2020; Thom & Turner, 2020). This in turn creates an additional barrier to healthcare access due to the intense discomfort hypersensitive individuals may feel while wearing masks. Providers can mitigate these discomforts by allowing such patients to choose the kind of mask they prefer, such as fabric or cotton. (B) For individuals who struggle with eye contact in social situations, masks again exacerbate symptoms by pushing one’s focus onto another’s eyes (Thom & Turner, 2020). (C) Individuals who are hard-of-hearing and use lip reading as a source of communication will struggle to interact with care providers (Kohek et al., 2020; Pendo et al., 2020). Although there are transparent masks that partially alleviate this problem (Pendo et al., 2020), many medical facilities do not routinely carry these. (D) Individuals with physical impairments could encounter difficulty with the dexterity involved in putting on and removing their masks (Kohek et al., 2020; Pendo et al., 2020). Although restricting the number of people in confined spaces is important during the pandemic, providers should consider allowing these patients to bring in a caregiver or aid. (E) A subgroup of individuals with developmental disabilities may experience difficulties breathing when wearing a mask (Kohek et al., 2020; Pendo et al., 2020). One study found that children with disabilities were 10% (n=71,811) more likely to be diagnosed with asthma compared to able-bodied peers, which is reflective of asthma’s well- established association as a common comorbidity with many developmental disabilities, such as ASD (Xie et al., 2020).
(3) COVID-19 Testing
While some studies have considered challenges pertaining to COVID-19 testing of patients with disabilities, further examination is warranted. First, accessing COVID-19 testing locations can be problematic for special needs patients (Constantino et al., 2020). For example, individuals with physical disabilities may require a wheelchair transport, which has become less available due to recent closures of driving service businesses with special medical transport equipment. Secondly, the preferred COVID-19 testing regimen involves moderately uncomfortable deep nasopharyngeal swabs. As previously mentioned, there is a subset of people with intellectual disabilities that have hypersensitivity to touch, including those with ASD. For these patients such exams can be traumatic (Thom & Turner, 2020). To help prepare such patients for this uncomfortable experience, showing a video or picture book demonstration may prove useful. In addition, the provider could also ask if the patient has any activities they use to calm down, such as listening to music or squeezing a stress ball (Thom & Turner, 2020). The new, less invasive, saliva-based COVID-19 testing method will theoretically cause fewer problems for patients with sensory issues; however, no relevant research could be found as of writing.
(4) The Patient-Physician Relationship (PPR)
Telemedicine and face-obstructing personal protective equipment are generally thought to decrease the personal connection between patient and physician (Hooshmand & Foronda, 2017; Lapow, 2020). Online healthcare diminishes the personal component while mask-wearing decreases the ability of both individuals to read social cues by interpreting facial expressions (Lapow, 2020). Providers must consequently adjust their skillset to facilitate virtual trust and empathy while interpreting subtle body language (Mann et al., 2020). To date, there has been a lack of inquiry into how these COVID-19-related healthcare delivery changes affect the PPR for individuals with disabilities, but pre-COVID-19 research can be used to conceptualize how the effects of these changes may unfold (Constantino et al., 2020).
The disabled community is a complex and heterogeneous population. Pre- pandemic research indicates that the use of telemedicine has differential and inconsistent effects on various segments of this community. For example, telemedicine will negatively impact the PPR for special needs individuals who are non-verbal and communicate mainly via gestures. The use of online technology could impact the physician’s ability to view these gestures, interpret them effectively, and respond appropriately (Chew et al., 2009). However, patients can have in-home communication devices readily available to them to increase ease of interaction between patient and physician (Hemsley et al., 2012). For these individuals, the use of masks during in- person visits may not impede an effective PPR, as they will still be able to communicate their needs through physical signals.
Non-COVID-19-related research suggests that diversifying providers’ rapport- building skills to include the reading of cues through remote or masked consultation will incur benefits for a subset of people with disabilities. Individuals with intellectual disabilities like ASD may exhibit inappropriate social cues as well as the inability to interpret the cues of others (Dimitrovsky et al., 1998; Eshraghi et al., 2020; Sheppard et al., 2016). Research suggests that during human interactions, each person naturally assumes that those involved can accurately evaluate one’s own social presentation and will read facial expressions similarly to oneself (Matsumoto & Hwang, 2011). Without proper training or experience, medical providers may encounter misunderstandings when interacting with intellectually disabled individuals who produce inappropriate social expressions and readings of others’ cues (Dimitrovsky et al., 1998; Eshraghi et al., 2020; Sheppard et al., 2016). As such, COVID-19 has generated incentives for providers to create the best possible PPR in the absence of clear social signals.
Conclusion
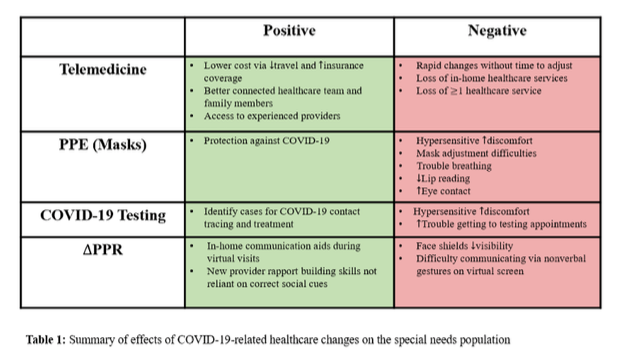
In summary, all four of these major COVID-19 responses to healthcare delivery have had adverse short-term effects on individuals with disabilities, while telemedicine and PPR have shown potential positive long-term implications as well (Table 1). Much of this paper’s analysis is built on pre-COVID-19 studies that must be extrapolated and reapplied to pandemic-era conditions. In addition, the scarce research that has so far been conducted has placed an emphasis on children with special needs, while adult populations have garnered less attention. The work that has been done reveals a need for investigators to increasingly study the uneven effects of COVID-19-related healthcare delivery changes on the special needs community. Illuminating this imbalance would help to include the interests of patients with disabilities in the conversation regarding the structure of healthcare delivery during unique public health situations.
Download PDF
References
Aishworiya, R., & Kang, Y. Q. (2020). Including Children with Developmental Disabilities in the Equation During this COVID-19 Pandemic. Journal of Autism and Developmental Disorders, 1–4.
Annaswamy, T. M., Verduzco-Gutierrez, M., & Frieden, L. (2020). Telemedicine barriers and challenges for persons with disabilities: COVID-19 and beyond. Disability and Health Journal, 13(4), 100973.
Anthony Jnr, B. (2021). Implications of telehealth and digital care solutions during COVID-19 pandemic: A qualitative literature review. Informatics for Health & Social Care, 46(1), 68–83.
Boyle, C. A., Fox, M. H., Havercamp, S. M., & Zubler, J. (2020). The public health response to the COVID-19 pandemic for people with disabilities. Disability and Health Journal, 13(3), 100943.
Chaudhry, H., Nadeem, S., & Mundi, R. (2021). How Satisfied Are Patients and Surgeons with Telemedicine in Orthopaedic Care During the COVID-19 Pandemic? A Systematic Review and Meta-analysis. Clinical Orthopaedics and Related Research, 479(1), 47–56.
Chew, K. L., Iacono, T., & Tracy, J. (2009). Overcoming Communication Barriers: Working with Patients with Intellectual Disabilities. Australian Family Physician, 38(1/2), 10.
Constantino, J. N., Sahin, M., Piven, J., Rodgers, R., & Tschida, J. (2020). The Impact of COVID-19 on Individuals With Intellectual and Developmental Disabilities: Clinical and Scientific Priorities. American Journal of Psychiatry, 177(11), 1091–1093.
Dimitrovsky, L., Spector, H., Levy-Shiff, R., & Vakil, E. (1998). Interpretation of facial expressions of affect in children with learning disabilities with verbal or nonverbal deficits. Journal of Learning Disabilities, 31(3), 286–292, 312.
Eshraghi, A. A., Li, C., Alessandri, M., Messinger, D. S., Eshraghi, R. S., Mittal, R., & Armstrong, F. D. (2020). COVID-19: Overcoming the challenges faced by individuals with autism and their families. The Lancet. Psychiatry, 7(6), 481–483.
Galanis, P., Vraka, I., Fragkou, D., Bilali, A., & Kaitelidou, D. (2021). Impact of personal protective equipment use on health care workers’ physical health during the COVID-19 pandemic: A systematic review and meta-analysis. MedRxiv, 2021.02.03.21251056.
Gao, Y., Liu, R., Zhou, Q., Wang, X., Huang, L., Shi, Q., Wang, Z., Lu, S., Li, W., Ma, Y., Luo, X., Fukuoka, T., Ahn, H. S., Lee, M. S., Luo, Z., Liu, E., Chen, Y., Shu, C., & Tian, D. (2020). Application of telemedicine during the coronavirus disease epidemics: A rapid review and meta-analysis. Annals of Translational Medicine, 8(10).
Hemsley, B., Balandin, S., & Worrall, L. (2012). Nursing the patient with complex communication needs: Time as a barrier and a facilitator to successful communication in hospital: ‘Time’ and communication in hospital. Journal of Advanced Nursing, 68(1), 116–126.
Hooshmand, M., & Foronda, C. (2017). Comparison of Telemedicine to Traditional Face-to-Face Care for Children with Special Needs: A Quasiexperimental Study. Telemedicine and E-Health, 24(6), 433–441.
Jeste, S., Hyde, C., Distefano, C., Halladay, A., Ray, S., Porath, M., Wilson, R. B., & Thurm, A. (2020). Changes in access to educational and healthcare services for individuals with intellectual and developmental disabilities during COVID-19 restrictions. Journal of Intellectual Disability Research, 64(11), 825–833.
Karp, W. B., Grigsby, R. K., Dsw, L., McSwiggan-Hardin, M., Pursley- Crotteau, S., Carn§, Adams, L. N., Bell, W., Stachura, M. E., & Kanto, W. P. (2000). Use of Telemedicine for Children With Special Health Care Needs. Pediatrics, 105(4), 843–847.
Kohek, J., Seth, A., Edwards, M., & Zwicker, J. (2020). Mandatory Mask Bylaws: Considerations Beyond Exemption for Persons with Disabilities. The School of Public Policy Publications 2020, 13.
Lapow, J. (2020). Telemedicine, PPE, and COVID-19: A New Paradigm for the Patient-Physician Relationship. The Roundtable Journal on Health Policy, 3(1), 8.
Lebrasseur, A., Fortin-Bédard, N., Lettre, J., Bussières, E.-L., Best, K., Boucher, N., Hotton, M., Beaulieu-Bonneau, S., Mercier, C., Lamontagne, M.-E., & Routhier, F. (2021). Impact of COVID-19 on people with physical disabilities: A rapid review. Disability and Health Journal, 14(1), 101014.
Mann, D. M., Chen, J., Chunara, R., Testa, P. A., & Nov, O. (2020). COVID-19 transforms health care through telemedicine: Evidence from the field. Journal of the American Medical Informatics Association, 27(7), 1132– 1135.
Matsumoto, D., & Hwang, H. S. (2011). Reading facial expressions of emotion. Psychological Science Agenda, 25(5).
Monaghesh, E., & Hajizadeh, A. (2020). The role of telehealth during COVID-19 outbreak: A systematic review based on current evidence. BMC Public Health, 20(1), 1193.
Neece, C., McIntyre, L. L., & Fenning, R. (2020). Examining the impact of COVID-19 in ethnically diverse families with young children with intellectual and developmental disabilities. Journal of Intellectual Disability Research, 64(10), 739–749.
Pendo, E., Gatter, R., & Mohapatra, S. (2020). Resolving Tensions between Disability Rights Law and COVID-19 Mask Policies. Maryland Law Review Online, 80, 1.
Robinson, S. S., Seale, D. E., Tiernan, K. M., & Berg, B. (2003). Use of telemedicine to follow special needs children. Telemedicine Journal and E-Health: The Official Journal of the American Telemedicine Association, 9(1), 57–61.
Sheppard, E., Pillai, D., Wong, G. T.-L., Ropar, D., & Mitchell, P. (2016). How Easy is it to Read the Minds of People with Autism Spectrum Disorder? Journal of Autism and Developmental Disorders, 46(4), 1247–1254.
Sivaraman, M., Virues-Ortega, J., & Roeyers, H. (2020). Telehealth mask wearing training for children with autism during the COVID -19 pandemic. Journal of Applied Behavior Analysis, 10.1002/jaba.802.
Teräs, M., Suoranta, J., Teräs, H., & Curcher, M. (2020). Post-Covid-19 Education and Education Technology ‘Solutionism’: A Seller’s Market. Postdigital Science and Education, 2(3), 863–878.
Thom, R., & Turner, K. (2020, June 10). Helping people with autism spectrum disorder manage masks and COVID-19 tests. Retrieved from Harvard Health Blog. https:// http://www.health.harvard.edu/blog/ helping-people-with-autism- spectrum-disorder-manage-masks- and-covid-19-tests-2020061020089
Xie, L., Gelfand, A., Delclos, G. L., Atem, F. D., Kohl, H. W., III, & Messiah, S. E. (2020). Estimated Prevalence of Asthma in US Children With Developmental Disabilities. JAMA Network Open, 3(6), e207728–e207728.
